



Recent News

Funding for A Healthier World
UHN researchers received over $20.7 million in CIHR’s Spring 2026 Project Grant competition.
Read MoreFunding for A Healthier World
UHN researchers received over $20.7 million in CIHR’s Spring 2026 Project Grant competition.
UHN researchers have secured more than $20.7 million in total funding from the Canadian Institutes of Health Research (CIHR) Spring 2026 Project Grant Competition. This round of funding will support 26 projects advancing discoveries and innovations at UHN.
Nationally, 439 research grants were awarded, representing a total investment of approximately $412 million. In addition, 19 priority announcement grants, totaling $1.9 million, and 9 supplemental prizes, totaling $305,000, were awarded.
At UHN, this research will explore new treatments and ways to improve patient outcomes. Funded projects include investigating the use of blood tests to analyze treatment resistance in small-cell lung cancer (led by Dr. Benjamin Lok) and the ability of brain imaging to predict whether patients with Parkinson disease will benefit from deep brain stimulation (DBS) (co-led by Dr. Alexandre Boutet). Another study will use AI-driven methods to optimize lab-grown heart tissues to help reduce inflammation and support less invasive treatments for repairing damage heart muscle (led by Dr. Milica Radisic).
Additional studies will focus on advancing health outcomes across diverse populations through innovative and targeted research. One research team is aiming to improve patient surveys for First Nations Peoples to better reflect their lived experiences (co-led by Dr. Istvan Mucsi). Another upcoming project will evaluate whether specific drug combinations can improve kidney health in people with type 2 diabetes and albuminuria, a condition in which excess protein (albumin) leaks into the urine and can indicate kidney damage (co-led by Dr. David Cherney). Other research will test balance function in older adults with hearing loss, providing deeper insights into age-related changes in hearing and balance (co-led by Dr. Jennifer Campos).
This funding will support UHN's commitment to research and innovation, enabling discoveries that drive meaningful advancements in health care and contribute to A Healthier World. Thank you to CIHR for its support and congratulations to all awardees!
See the full list of the awarded projects here.
×

Research Spotlight
Read the latest bi-monthly newsletter that highlights advancements from UHN researchers.
Read MoreResearch Spotlight
Read the latest bi-monthly newsletter that highlights advancements from UHN researchers.
Welcome to the latest issue of Research Spotlight.
As Canada’s largest research hospital, UHN is a national and international source for discovery, education, and patient care. This newsletter highlights top research advancements from over 5,000 members of TeamUHN—a diverse group of trainees, staff, and principal investigators who conduct research at UHN.
Stories in this month’s issue:
● Hearing, Balance, and Thinking: Cognitive training improves balance and multitasking with varied benefits to hearing ability.
● Guiding Equal Heart Failure Care: Study finds new strategy for heart failure care is equally effective for males and females.
● Brain Stimulation to Treat OCD: Large-scale UHN-led study finds brain stimulation treatments may help people with severe OCD
● New Clues to Leukemia Relapse: Researchers uncover how DNA elements may fuel leukemia recurrence and therapy resistance.
Read these stories and more online here. To read previous issues, see the newsletter archive.
×

Retaining a Vital Nursing Workforce
Clearer roles and stronger career support could help retain registered practical nurses.
Read MoreRetaining a Vital Nursing Workforce
Clearer roles and stronger career support could help retain registered practical nurses.
Image Caption: Registered practical nurses are playing an increasingly important role in Canadian hospitals, highlighting the need for role clarity, professional development opportunities, and workplace supports that promote retention.
In response to persistent nursing shortages post-pandemic, hospitals across Canada have increasingly relied on registered practical nurses (RPNs) to help meet growing patient care needs. A new study from The Institute for Education Research at UHN suggests that as RPNs take on expanded responsibilities in care settings, clearer role expectations, stronger professional development opportunities, and improved workplace supports are needed to improve retention and strengthen collaboration.
In Canada, both RPNs and registered nurses (RNs) are licensed nurses, but RNs complete more extensive education and are more common in hospital settings. Traditionally, RNs care for patients with more complex or unpredictable health needs, while RPNs care for patients in more stable conditions. However, with ongoing staffing shortages, RPNs’ roles continue to evolve and grow. To better understand the unique role of RPNs and how they work alongside other health care team members, the research team interviewed 24 participants, including RNs, RPNs, nurse leaders, and personal support workers in hospital care settings.
Participants described teamwork, cross-team collaboration, and clear communication as essential during key care decision points and in managing increasingly complex patient care needs. However, many participants expressed uncertainty about the boundaries between RN and RPN responsibilities, particularly when patient conditions changed or became more complex. Participants identified a need for greater role clarity and more consistent guidance from both nursing regulatory agencies and health care organizations.
Participants also acknowledged the value of the RPN role in providing an accessible entry point to the nursing profession and supporting a cost-effective staffing model for organizations. However, these benefits also highlight the need for more targeted strategies for retaining RPNs, including appropriate compensation and opportunities for career advancement.
The findings suggest that hospitals and nursing regulatory bodies could improve collaboration and retention by providing clearer guidance on nursing roles and creating more opportunities for professional growth. As health care systems continue to evolve, supporting the retention and development of RPNs may be an important step toward maintaining high-quality patient care and building a more sustainable nursing workforce.
Dr. Alyssa Indar, lead author of the study, is an Education Investigator at The Institute for Education Research at UHN. Dr. Indar is also an Adjunct Lecturer at the Lawrence Bloomberg Faculty of Nursing at the University of Toronto.
Dr. Sherry Espin, co-author of the study, is an Affiliate Scientist at The Institute of Education Research at UHN. Dr. Espin is also a Professor in the Daphne Cockwell School of Nursing at Toronto Metropolitan University.
This work was supported by UHN Foundation and the Registered Practical Nurses Association of Ontario (WeRPN).
Indar A, Espin S, Jones A, Bookey-Bassett S, Martina K, Hubley P, Teodoro J, Aiello M, Browne C. Intraprofessional collaboration in acute care: Generating evidence to inform nursing workforce retention strategies. Nurs Outlook. 2026 Jun 11. doi: 10.1016/j.outlook.2026.102832.
×
Understanding Spine Surgery Outcomes
Study finds overall osteoarthritis burden may influence recovery after lumbar spine surgery.
Read MoreUnderstanding Spine Surgery Outcomes
Study finds overall osteoarthritis burden may influence recovery after lumbar spine surgery.
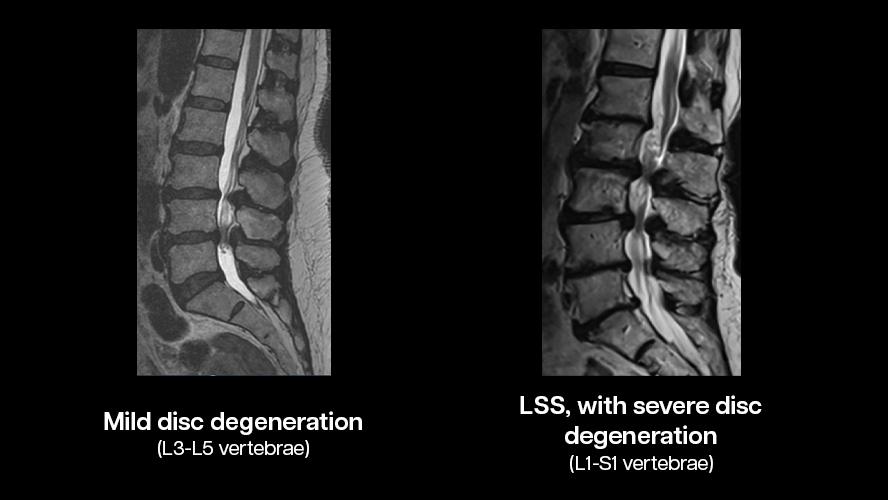
Image Caption: Osteoarthritis (OA) affects nearly 15% of all Canadians. Although OA in the spine is common, most research is focused on OA in appendage joints, such as knees, hands, and hips. For those with spinal OA, the symptoms can be debilitating, seriously impairing quality of life. (Original images c/o UHN's Schroeder Arthritis Institute)
New research from UHN's Schroeder Arthritis Institute suggests that patients with more extensive lumbar disc degeneration may be less likely to benefit from surgery for lumbar spinal stenosis, a narrowing of the spinal canal in the lower back, caused by osteoarthritis (LSS-OA). The findings could help surgeons and patients make more informed treatment decisions and set realistic expectations before surgery.
LSS occurs when osteoarthritis and age-related changes in the spine narrow the space around nerves in the lower back, causing symptoms such as pain, numbness, weakness, and difficulty walking. Surgery is designed to decompress the spine and relieve pressure on these nerves. However, up to 40% of patients do not experience meaningful improvement after surgery.
To better understand this disparity in outcomes, the researchers analyzed data from 119 patients who underwent surgery for LSS-OA. Using MRI scans, the team assessed the extent of disc degeneration throughout each patient's lumbar spine. Before surgery and one year afterward, patients’ pain scores and level of disability were assessed through various questionnaire-style assessments. Participants also self-reported OA symptoms in other joints.
Dr. Raja Rampersaud, the first author of this study, and his colleagues found that about 25% of patients had a high burden of lumbar disc degeneration. Of these patients, only 50% achieved a clinically meaningful improvement in disability after surgery. In contrast, nearly 75% of patients with lower levels of degeneration achieved meaningful improvement.
The study also showed that many patients experienced symptoms beyond the spine. More than half reported pain or stiffness in at least three other joint sites, such as the hips, knees, hands, or feet. Patients with greater joint involvement experienced less improvement after surgery.
Together, the findings suggest that surgical outcomes may depend on both the condition of the surgical site and the overall burden of OA throughout the spine and the rest of the body. A more comprehensive view of OA and musculoskeletal health could support more personalized treatment planning and improve outcomes for those living with LSS-OA.
Dr. Raja Rampersaud, Krembil Clinician Investigator at UHN’s Schroeder Arthritis Institute and Professor in the Department of Surgery at the University of Toronto’s Temerty Faculty of Medicine, is the first author.
Dr. Anthony Perruccio, Senior Scientist at UHN’s Schroeder Arthritis Institute, is the senior author. He is also a Professor at the University of Toronto’s Institute of Health Policy, Management and Evaluation (IHPME), Dalla Lana School of Public Health, and Temerty Faculty of Medicine Department of Surgery.
This work was supported by the J. Bernard Gosevitz Chair in Arthritis Research and UHN Foundation. Dr. Perruccio was supported directly by an award from the Arthritis Society Canada.
Dr. Rampersaud receives royalties from Medtronic outside of the work in this study, and Dr. Kapoor is an Executive Board Member, Treasurer, and President-Elect of the Osteoarthritis Research Society International (OARSI) as well as a Scientific Advisory Board Member for Chiron Inc.
Rampersaud YR, Power JD, Nahanni C, Fine N, Canizares M, Kapoor M, Perruccio AV. The impact of overall lumbar disc degeneration burden on disability outcomes following surgery for lumbar spinal stenosis due to osteoarthritis. Osteoarthr Cartil Open. DOI: 10.1016/j.ocarto.2026.100766.
×

Meet Dr. Benjamin Haibe-Kains @PMResearch
Making AI research transparent for a safe health care system
Read MoreMeet Dr. Benjamin Haibe-Kains @PMResearch
Making AI research transparent for a safe health care system
Image Caption: Dr. Benjamin Haibe-Kains is UHN’s Executive AI Scientific Director and Co-Director, UHN AI Hub, Senior Scientist and Allan Slaight Scientist at UHN’s Princess Margaret Cancer Centre, and Scientific Director of the Cancer Digital Intelligence Program at Princess Margaret Cancer Centre.
Dr. Benjamin Haibe-Kains was completing his PhD when a major cancer research scandal shook the scientific community.
A highly publicized study claiming to predict patients’ responses to chemotherapy was later found to be based on manipulated data, leading to retracted papers, suspended clinical trials and years of wasted research effort.
Watching the case unfold and seeing the consequences profoundly influenced Benjamin’s approach to science. “I suddenly realized that if I'm not being completely open and transparent about what I do and if I make mistakes, it could take years for people to correct them and do what’s right for patients,” he recalls. “And for me, that was not an acceptable risk. So, I decided to invest my effort in the principles of open science.”
Today, with many leadership roles at UHN and its Princess Margaret Cancer Centre (PM), Benjamin is helping shape how artificial intelligence is developed and deployed in health care research, advocating for approaches that are not only innovative, but also trustworthy, transparent, and beneficial to patients.
Guardrails for developing AI models
“Every year, hundreds of studies are published describing predictive models for cancer care, but very few ever make the leap into clinical practice,” says Benjamin. “Pursuing a wrong model not only wastes time and resources, but could also negatively impact patient care.”
This troubling trend prompted Benjamin and a group of international collaborators to set up an industry standard—the Seven Hallmarks of Predictive Oncology—designed to evaluate the quality, reliability, and clinical potential of AI models before they reach the bedside.
“We use these hallmarks to identify models with the greatest potential for clinical translation and to minimize risks before they enter hospitals,” Benjamin explains.
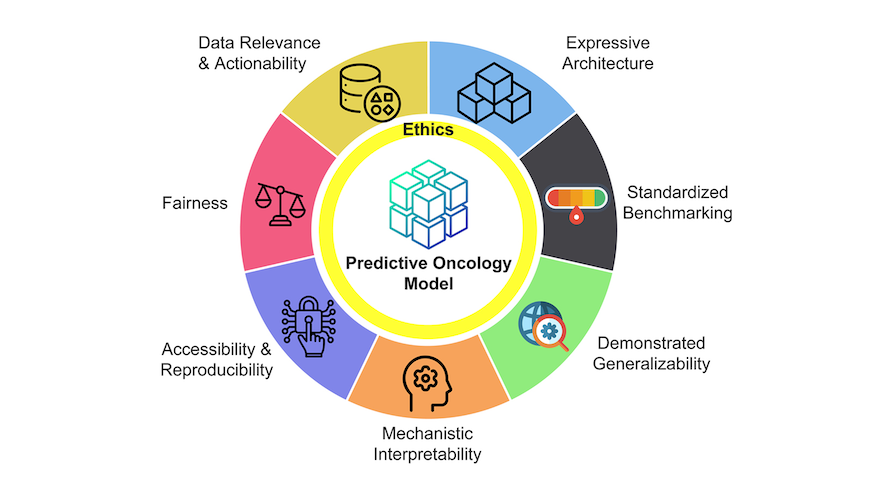
The seven hallmarks of predictive oncology (Graphic credit to Singhal et al., Cancer Discovery AACR Journal)
Together, the hallmarks assess whether a model is built on data that are relevant to patient care and available in real-world settings; whether the design is complex enough to capture the biology of cancer without overfitting the data; whether it has been rigorously benchmarked against existing approaches; whether the study can make accurate predictions for new patients beyond the population on which it was trained; whether clinicians can understand the factors driving its predictions; whether other researchers can reproduce its results; and whether it performs equitably across diverse patient populations and not just groups represented in the training data.
In addition to scientific rigour, each hallmark carries important ethical considerations. “If you push a model that is not sufficiently accurate, you may waste precious health care resources and reduce the likelihood of patient benefit,” he explains. “Ethical considerations must be embedded in every step of AI development.”
Using computational science for cancer discoveries
Cancer research was not part of Benjamin’s original career plan. He studied computer science at the Université Libre de Bruxelles and was initially interested in robotics. His path changed when a supervisor introduced him to the emerging field of bioinformatics.
“That’s when I started to work with clinicians,” Benjamin recalls. “I got hooked by the fact that I could be working to help the patients at the end of the day.”
Working alongside cancer biologists, bioengineers, and clinicians during his PhD, he learned the language of cancer research while applying computational approaches to uncover previously unknown subtypes of breast cancer.
Benjamin later pursued postdoctoral training to develop more sophisticated computational methods, moving beyond simply applying existing ones. At the Harvard School of Public Health and Dana-Farber Cancer Institute, he studied how genes interact in complex networks, deepening his expertise in machine learning and predictive oncology.
After joining Princess Margaret in 2013, Benjamin led a landmark study with collaborators at the Université de Montréal to better understand why some patients respond to immunotherapy while others do not. The team assembled data from 26 clinical trials spanning 12 cancer types and three classes of immunotherapies, bringing together molecular profiles and treatment outcomes from more than 3,600 patients.
“We analyzed each gene individually to determine whether it could predict response to immunotherapy,” Benjamin explains. “This led us to identify a 100-gene signature that was more predictive than previously published approaches across multiple cancer types.”
The team identified two promising new immunotherapy targets by examining the functions of the genes in the signature. The targets are currently being investigated by study co-lead Dr. John Stagg, Director of the McGill Goodman Cancer Centre.
“I have always enjoyed collaborating with scientists around the world, but the highly collaborative culture of Canadian research makes these partnerships especially rewarding and productive,” Benjamin says.
Bringing AI to clinical settings
Benjamin co-leads PM’s Cancer Digital Intelligence (CDI) program with radiation oncologist Dr. Alejandro Berlin to smoothly translate AI technologies into clinical application.
“What we are trying to do is to build a bridge between research and clinical application and foster more innovations within the institute.”
One example is a predictive model developed by Dr. Robert Grant’s team to identify cancer patients who are likely to return to the emergency department for treatment-related complications. CDI helped refine the model and support its deployment in the clinic, where it is currently being evaluated in a “shadow mode” environment alongside routine clinical care.
Another flagship CDI initiative is PMATCH, an AI-enabled platform designed to connect patients with relevant clinical trials more efficiently. The system automatically extracts key information from patient records, evaluates it against trial eligibility criteria, and alerts clinicians to potential matches. Now operating as a pilot at Princess Margaret, PMATCH processes data from more than 200 patients each week, with plans to expand the platform beyond Ontario.
“We want to see whether this technology can be used across multiple hospitals, to help more patients access clinical trials regardless of where they receive care,” Benjamin says.
Humans have a lot to give in this AI-driven world
When it comes to concerns about the rapid pace at which artificial intelligence is transforming society, Benjamin's advice is to embrace the technology while understanding its limitations.
“We need to learn how to use these tools effectively without giving up on our own creativity or judgment,” he says.
Benjamin believes AI excels at finding unexpected connections across different fields because of its broad knowledge base. What it struggles to replicate, he argues, is the kind of disruptive creativity from people who challenge conventional thinking and pursue entirely new directions. He cites examples like Albert Einstein and Marie Curie, iconoclasts whose transformative discoveries fundamentally changed how people understood the world.
“There will be an interplay between the creativity of humans trying to think out-of-the-box, and the creativity of AI to connect the dots in various fields.”
Specifically, biomedical research is entering a new era with the rise of AI co-scientists and automated laboratories. “We are at the stage to reimagine the scientific process where AI and human capabilities complement and strengthen one another,” says Benjamin. “Researchers who adapt and harness the potential of these technologies will be well positioned to shape what comes next and drive future innovation.”
Trust will play a critical role in the health care system. “AI may work 90 per cent of the time, but for the remaining 10 per cent, if humans are not in the loop and people don't trust the system anymore, there is no way we can fix the problem,” he says.
For that reason, he underscores the effort to assess the quality, reliability, and robustness of AI-related technologies before they can be used in a safe and responsible way in the clinic.
“Human-in-the-loop will remain essential for a long time,” he says. “Many complex health care decisions cannot be fully driven by AI. Clinicians, administrators, nurses and other health care professionals will continue to play a crucial role in the responsible use and evaluation of these new technologies.”
Meet PMResearch is a story series that features Princess Margaret researchers. It showcases the research of world-class scientists, as well as their passions and interests in career and life—from hobbies and avocations to career trajectories and life philosophies. The researchers that we select are relevant to advocacy/awareness initiatives or have recently received awards or published papers. We are also showcasing the diversity of our staff in keeping with UHN themes and priorities.
×

Assessing Kidney Disease Globally
Kidney disease worsens outcomes for patients hospitalized with cirrhosis; study finds.
Read MoreAssessing Kidney Disease Globally
Kidney disease worsens outcomes for patients hospitalized with cirrhosis; study finds.
Image Caption: Chronic kidney disease, a progressive condition in which the kidneys lose their ability to function properly, is a growing global health concern. It can progress to end-stage kidney failure requiring dialysis or kidney transplant.
The global prevalence of chronic kidney disease (CKD) is increasing, leading to higher mortality among affected individuals and placing a growing burden on health care systems. A large international study co-led by UHN examined the prevalence and impact of CKD in those with cirrhosis—permanent scarring and damage of the liver. The researchers found that CKD negatively impacts the prognosis of patients with cirrhosis in a global cohort.
CKD occurs when the kidneys are damaged or do not function as they should for a prolonged period of time. It was once thought to be uncommon in patients with cirrhosis. However, its prevalence has increased among those with advanced liver disease. Experts say this increase is being driven by growing rates of other co-occurring metabolic conditions such as obesity, diabetes, and high blood pressure, as well as broader diagnostic criteria that identify CKD earlier.
However, most evidence on CKD in cirrhosis comes from Western countries, with minimal reporting from Africa, South America, or Oceania. To assess the global prevalence of CKD in cirrhosis and its impact on patient outcomes, the research team analyzed data from more than 7,000 hospitalized patients with cirrhosis enrolled in the Chronic Liver Disease Evolution and Registry for Events and Decompensation (CLEARED) consortium.
The study found that approximately 18% of people hospitalized with cirrhosis also had CKD. Rates were highest in high-income countries, where metabolic syndrome—a cluster of conditions that includes obesity, diabetes, high blood pressure, high cholesterol and fatty liver disease—is more common.
In patients with cirrhosis, CKD was more likely seen in those with ascites, a liver complication caused by a build-up of fluid in the abdomen. Patients with both CKD and cirrhosis also had more complex liver complications. Acute kidney injury (AKI), a sudden decline in kidney function, was the most common complication during hospitalization. It affected nearly 60% of patients with CKD, more than double the rate seen in patients without CKD. Patients in the hospital with both CKD and cirrhosis also had a higher risk of death during or shortly after hospitalization.
The results show that CKD negatively impacts outcomes for patients with cirrhosis, highlighting the need for closer monitoring and treatment of kidney disease in these patients. Careful management of ascites and lifestyle changes aimed at reducing risk factors could help improve outcomes, particularly in high-income countries.
Dr. Florence Wong is an Affiliate Scientist at UHN’s Organ Systems and Integrated Health Sciences Research Institute and a Professor in the Department of Medicine at The University of Toronto. She is the lead and corresponding author of the study.
This research was supported by UHN Foundation.
Wong F, Adebayo D, George J, Idilman R, Hayes PC, Alvares-da-Silva MR, Torre A, Mekonnen HD, Seto WK, Sarin SK, Cao Z, Rajoriya N, Nagral A, Fisseha H, Kulkarni AV, Zhu C, Debzi N, Farias AQ, Su M, Goel A, Marciano S, Livingstone R, Dhiman RK, Gao Y, Malé-Velázquez R, Demitars CO, Bera C, Jiang YF, Velarde-Ruiz Velasco JA, Tan HK, Zhao C, Huezo MSG, Asrani SK, Wang L, Lu M, Michalczuk MT, Barutcu S, Cordova-Gallardo J, Gofton C, Gounder M, Shaw J, Albhaisi S, Zheng X, Aravinthan A, Rajaram RB, Jothimani D, Thanapirom K, Benitez C, Dincer D, Saraya A, Xu B, Lin M, Wu X, Liu C, Reddy R, Bush B, Thacker LR, Topazian M, Xie Q, Silvey S, Kamath PS, Choudhury A, Bajaj JS; CLEARED Investigators. Chronic kidney disease in cirrhosis: a study of inpatients from a global perspective. Gut. 2026 Jun 5. doi: 10.1136/gutjnl-2025-336802. Epub ahead of print.
×

Creating Roadmaps to Better Care
Study explores what patients and caregivers identify as priorities for improved hospital stays.
Read MoreCreating Roadmaps to Better Care
Study explores what patients and caregivers identify as priorities for improved hospital stays.
Image Caption: Patient and caregiver input can help guide improvements to the quality of care in general medicine wards, potentially enhancing the experiences and health outcomes of many patients.
General medical wards in hospitals provide care to large and growing numbers of patients. As a result, identifying effective ways to improve the quality of care can enhance the experiences and outcomes of many individuals. A new study from UHN and the University of Toronto is shedding light on what matters most to patients and caregivers during a hospital stay, revealing that better communication, fewer delays, and greater inclusion in care decisions are among the top priorities for improvement.
By using an open-ended, multi-step approach, known as group concept mapping, researchers led by Dr. Lauren Lapointe-Shaw, Staff Physician in General Internal Medicine and Scientist at UHN’s Organ Systems & Integrated Health Sciences Research Institute, sought to identify high-priority areas directly from patients' and caregivers' experiences.
Over 500 patients and caregivers from general medical wards at 10 Canadian hospitals (in Ontario, Nova Scotia, British Columbia, and Alberta) participated in this multiphase study between November 2023 and February 2025. Participants included people from groups that are often underrepresented in health research, such as non-English speakers, people experiencing homelessness, individuals with mental health conditions, and people living with dementia.
Patients and caregivers first told researchers what contributed to their inpatient experience, and then later rated and sorted the resulting experience statements. The sorting exercise resulted in six main themes: Environment and Facilities, Personal Support, Delays, Communication, Nutrition, and Inclusivity and Engagement.
Overall, patients’ and caregivers’ own negative inpatient experiences, many of them related to the hospital environment, did not correlate with what issues they prioritized for improvement. Instead, it was system-level concerns such as care delays, communication breakdowns, and lack of inclusivity that were seen as the most important to improve. One example of this is how rare but harmful events, such as perceived discrimination, were prioritized for improvement by many, despite few having experienced these directly. Notably, priorities for improvement were consistent across different patient and caregiver groups, even when their experiences varied.
Although negative experience ratings and priorities for improvement were not strongly correlated, the top-rated item was the same for both: having to wait a long time in the emergency department before getting a bed on the ward. This issue negatively affected many patients and was also identified as the highest priority for improvement.
The other highest-ranked priorities for improvement centered around communication, inclusivity, and engagement. For example, not having enough opportunities to speak with a doctor was another top priority for improvement.
“This study offers a patient-defined roadmap to guide quality improvement efforts on inpatient wards,” says Dr. Lapointe-Shaw. “Our findings also demonstrate that patients and caregivers can and do make a distinction between their own negative experiences and what they consider most essential to improve, for the benefit of all patients.”
Dr. Lauren Lapointe-Shaw is a Scientist at UHN’s Organ Systems & Integrated Health Sciences Research Institute, Research Director of the Myrna Daniels Seniors Emergency Medicine Centre at UHN, and Associate Professor in the Departments of Medicine & Institute of Health Policy, Management and Evaluation (IHPME) at the University of Toronto. She is the lead and senior author of the study.
This work was supported by the Canadian Institutes of Health Research, the PSI Foundation, the Sinai UHN Medical Organization, St Michael’s Hospital Academic Medical Organization, and UHN Foundation.
Lapointe-Shaw L, Salahub C, Lee M, Verma AA, Razak F, Ambasta A, Refaei M, Carpenter T, Moses B, Shetty N, Miller AP, Spicer E, Rawal S, Soong C, Kuluski K, Okrainec K, Baker GR, Chartier LB, Dhalla IA, Joseph R, Wodchis WP, Desveaux L, Wu W, Granieri M; GIM Priorities Group. Patient and caregiver priorities for quality improvement on general medical wards: a multicentre group concept mapping study. BMJ Qual Saf. 2026 Jul 19:bmjqs-2026-020280. doi: 10.1136/bmjqs-2026-020280. Epub ahead of print.
×
Research Institutes at UHN
Research conducted at UHN's research institutes spans the full spectrum of diseases and disciplines, including cancer, cardiovascular sciences, transplantation, neural and sensory sciences, musculoskeletal health, rehabilitation sciences, and community and population health.
Research Institutes
Research at UHN is conducted under the umbrella of the following research institutes. Click below to learn more:

